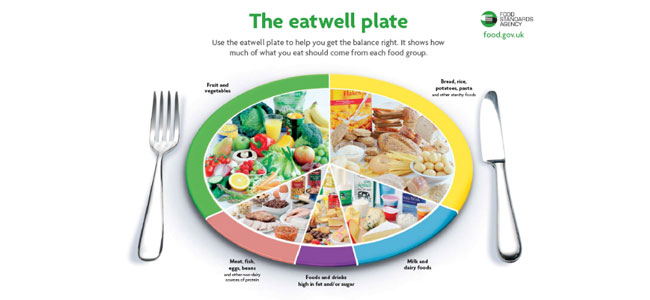
Image taken from: www.food.gov.uk/sites/default/files/multimedia/pdfs/nutrientinstitution.pdf
Here in the UK we have a major challenge with obesity. Every evening there is a programme on TV about obesity and weight loss, most of which concludes that the best approach is to staple around 90% of the stomach in order to aid fat loss.
Unfortunately the long term side effects of such surgery are rarely outlined. Reported side effects include:
Short Term
- Diarrhea
- Stomach Upsets
- Nausea
- Vomiting
- Heartburn
- Lethargy
- Hair loss
- Dry skin
Long term
- Nutritional Deficiencies – leads to unlimited health complications such as osteoporosis.
- Overeating may dislodge staples and cause death
- Nearly 90% of patients will end up with gallstones
How Fat is the UK?
In the national diet and nutrition surveys in 1986/87 and 2000/2001 the rate of obesity in men rose from 8% to 25% and in women 12% to 20% with 66% of men being classified at least overweight, that’s a 21% increase, along with 53% of women overweight a 17% increase since 1987 (1)
As a fat loss specialist in central London, the first logical question I would ask is “what have the eating habits been like in the UK during these time periods”. According to government experts increased fat intake will make you fat, so you would naturally assume that the fat consumption has increased between 1986-2001. In fact, quite the opposite is the case. Mainly due to extensive education built around low fat diets and increasing grain consumption, the levels of fat in the diet have declined and the levels of carbohydrate have increased. From the same survey a list of major changes in the diet between that time was drawn up. The more significant increases and decreases are in bold.
- More pasta, rice and other cereals
- More breakfast cereals
- More semi-skimmed milk
- More yoghurt and fromage frais
- More coated chicken and turkey
- More chicken and turkey
- Less Whole milk
- Less wholemeal bread
- Less puddings
- Less fat and oils
- Less butter
- Less liver and liver products
- Less other meats and meat products
The most significant change was that of the increased consumption of rice, pasta and other cereals, going from 236g per week to on average 507grams per week.
You would expect the authorities after a survey like this to ask themselves why more people are becoming obese and conditions associated with obesity are also on the rise, however this question has been ignored. Essentially the survey is being used to check whether the general public is following the recommendations set out, not whether the recommendations are right in the first place.
The Role of the British Nutrition Foundation (BNF)
The BNF are the main organisation in the UK that educate the public about nutrition and still there guidelines state:
- Eat more starchy foods such as breads, potatoes, rice and pasta.
- Choose leaner cuts of meat and lower fat dairy products that will help reduce the amount of fat, particularly saturated fatty acids in the diet (2).
The BNF provides advice to consumers, schools, government departments, health professions, the scientific community, and the media. It can be questioned however how impartial the BNF is when they receive funding from the food industry, just check some of the companies out for yourself. (3)
Who decides public nutrition recommendations?
It would be nice to assume that the organisations that feed information to us regarding nutrition are created with our best interests at heart. The scientific advisory committee on nutrition (SACN) are the main body involved with developing nutritional requirements for particular groups. The unfortunate truth is that many of the members have various ties with major food manufacturers, pharmaceutical companies and companies like weight watchers (4).
Why are Grains Making You Fat?
The consumption of grains in evolutionary terms is essentially a very recent thing, and whilst many people can tolerate grains, many of us have not genetically adapted to eating them (5). One of the main trouble makers is gluten that is contained in most grains. Many suffer damage to the intestinal lining from gluten containing grains, and recently research has shown gluten to be an issue with a whole host of conditions including:
- Reproductive Health
- Thyroid dysfunction
- Cognitive disorders
- Musculoskeletal disorders
- Immune Health
(6)
Inflammatory responses caused by such things as stress and reactions to foods can increase cortisol response which has been shown to increase fat storage around the mid section (7). This however is not the main reason excessive consumption of grains makes us fat.
- Protein and fat satisfy hunger more than carbohydrates and help reduce overall calorie intake. (8)
- Grains are much faster releasing into the body than proteins and fats. The increased speed of breakdown more rapidly increases blood sugar levels and thus increases in insulin secretion follow. If the muscles are not in need of the glucose or the cells are resistant to pulling in the glucose the excess glucose will be shifted to the fat stores and converted into fat.
- In a study of over 85,000 women between 1980 and 1990 the average glycemic load of their diet increased by 22%, during the same period the number of women who were overweight increased by 38%. (9)
So what works?
As a specialist in weight loss with a number of success stories, it is my view that individualised programme should be applied to every single client as some favour a low fat high carbohydrate based diet and others may favour a high fat and protein low carbohydrate based diet, it is not only variable from person to person but also variable for that individual depending on their current body shape activity levels and so forth. However numerous research studies have demonstrated that nutritional programmes with lower levels of carbohydrate and increased levels of fats and proteins produce a much higher success rate for fat loss (10-13), and this is something I would agree with for almost 90% of my clients.
Contact Steve Grant Health
To learn more out how Steve Grant Health can assist you on your journey, please fill out the enquiry form below.
Please note that depending on your specific circumstances and goals, Steve may recommend that you work with one of the specialist practitioners within his network of trusted professionals.
If you have been referred by a clinician, please complete the form and ensure that you state who has referred you or have your practitioner email Steve direct to make a referral that way.
Click the button below to open the client enquiry form:
[widgetkit id=”643″]
References
- The National Diet and Nutrition Survey: Adults aged 19 to 64, 2003. Office of National Statistics. Sourced from www.statistics.gov.uk/ssd/surveys/national_diet_nutrition_survey_adults.asp
- British Nutrition Foundation “Energy”. Statistics Sourced from http://www.britishnutrition.org.uk/home.asp?siteId=43§ionId=606&subSubSectionId=324&subSectionId=320&parentSection=299&which=1
- British Nutrition Foundation “BNF Member Companies” http://www.britishnutrition.org.uk/home.asp?siteId=43§ionId=352&parentSection=305&which=7
- Scientific Advisory Committee on Nutrition (SACN) Annual Report 2006 – Sourced from www.sacn.gov.uk/reports/
- Bray and Hoggan (2002) Dangerous Grains, Avery, New York
- Dr Tom O’Bryan, (2006) Unlocking the mystery of wheat and gluten sensitivity, literature review
- Purnel et al (2009) Enhanced cortisol production rates, free cortisol, and 11beta-HSD-1 expression correlate with visceral fat and insulin resistance in men: effect of weight loss, American Journal physiol Endocrinol Metab, Feb 292 (2)
- Brehm Et al (2003) A randomised trial comparing a very low carbohydrate diet and a calorie restricted low fat diet on body weight and cardiovascular riskfactors in healthy women, Journal of Endocrinology and Metabolism, 88 (4) 1617-1623
- Hu et al (2000) Trends in the incidence of coronary heart disease and changes in diet and lifestyle in women, New England Journal of Medicine, 343: 530-537
- Gardner CD, Kiazand A, Alhassan S, et al. (2007). “Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: the A TO Z Weight Loss Study: a randomized trial”. JAMA 297 (9): 969–77
- Foster et al (2003) A randomised trial of a low carbohydrate diet for obesity, New England Journal of Medicine, 348:2082-2090
- Yancy et al (2004) A low carbohydrate, ketogenic diet verses a low fat diet to treat obesity and hyperlipidemia, Annals of Internal Medicine 140:769-777
- Shai et al (2008) Weight loss with a low carbohydrate, Mediterranean or low fat diet, New England Journal of Medicine











